
GLAUCOMA
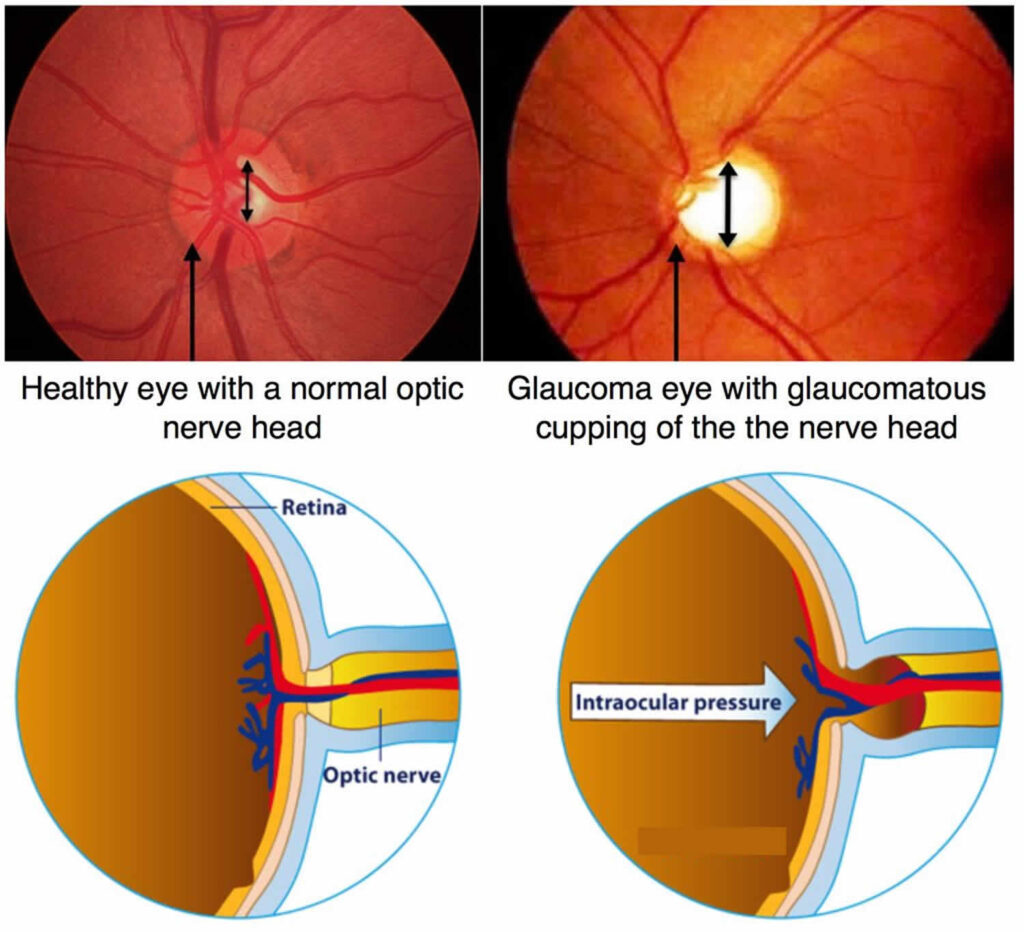
Glaucoma is a condition that causes the pressure inside the eye to be too high. If left untreated, this excessive pressure can damage the nerve that carries the vision to the brain; in severe cases, this can lead to blindness.
Different types of glaucoma
Glaucoma is divided into different subtypes. The thing that they all have in common is the damage to the optic nerve.
Primary Open Angle Glaucoma
The most common type of glaucoma is Primary Open Angle Glaucoma (POAG). The IOP (IntraOcular Pressure) may be higher than normal (normal range 10-21mmHg) but not always. The patient has no symptoms and it is discovered when the eye pressures are checked and found to be high or when the optician looks at the back of the eye and suspects that the optic nerve looks damaged in a particular pattern.
The human eyeball is a closed chamber in which fluid (aqueous) is produced and drained away constantly. This internal circulation of fluid within the eye is not the same as your tears. In POAG the drainage system does not filter the fluid sufficiently for reasons we still do not understand. Some people have optic nerves that are more susceptible to damage and in these patients even normal IOP can cause damage to the nerve. This may be because the blood supply to these susceptible optic nerves is compromised or the support for the optic nerve as it travels into the back of the eye is weak. Neither of these factors can be altered and so reducing the IOP in POAG is the only treatment option at the moment even if the starting IOP is within the normal range.
Angle Closure Glaucoma
In some patients the drainage channels that filter the aqueous within the eye are too small. As we all get older we develop cataracts and the evolving cataract can push against the drainage channels and make them smaller and narrower still. In some cases they can be blocked off altogether and the IOP rises acutely causing acute glaucoma. This is an ophthalmic emergency and urgent eye pressure reduction is required otherwise the vision will be lost forever.
It is important that the drainage angles are examined correctly when you see a glaucoma specialist. If we see narrow drainage angles before an acute attack occurs we can do a laser treatment to reduce the chances of an acute attack. This is called a ‘peripheral iridotomy.’ This is a tiny hole in the iris, the coloured part of your eye, akin to the hole at the top if your sink that stops the sink from overflowing. This is not a hole in the eye but is like an extra pupil at 12 o’clock in the iris. No one can see it and it is in a part of the iris that lies beneath the upper lid.
In some cases laser alone does not allow enough space for fluid to drain and it may be necessary to remove the growing cataract to restore the space for aqueous fluid to drain efficiently. This means that we sometimes operate on cataracts for IOP rather than for vision.
Secondary glaucoma
These are less common than POAG. In POAG we don’t yet know why the drainage channels stop working. In secondary glaucomas, there is an obvious reason for the rise in IOP.
1. Trauma
2. Rubeosis – abnormal blood vessels grow inside the eye due to diabetes, blocked veins or arteries inside the eye, poor blood supply in the carotid arteries in the neck. Rubeotic glaucoma is aggressive and almost always requires multiple surgical procedures.
3. Pseudoexfoliation – also known as PXF. PXF is seen as white powdery deposits on the lens, iris and drainage channels inside the eye. It can be associated with very high IOP and glaucoma that progresses very quickly. Early treatment and close follow up are essential.
4. Pigmentary glaucoma – this occurs when the iris rubs against the human lens that lies close behind it. This ‘rubbing’ dislodges the pigment that gives our eyes their colour. The pigment then clogs up the drainage channels leading to raised IOP and glaucoma. It particularly affects younger short -sighted people. Pigment shedding can often increase significantly during exercise.
5. Previous eye surgery. Previous retinal detachment surgery involving silicone oil increases the risk of glaucoma.
6. Inflammation. Patients who have chronic and repetitive inflammation in their eyes can develop glaucoma. This may be due to inflammatory related scarring of the drainage channels themselves or may be a response to the steroid drops that are necessary to treat inflammation.
Glaucoma causes
There is a higher risk of having an earlier onset and more severe glaucoma if you are:
•Of Black African origin;
•Have a close relative with glaucoma;
•Short-sighted;
•Diabetic;
•Have high eye pressure.